Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a chronic, debilitating systemic disease involving dysfunction of the neurological, vascular, immune, autonomic, and energy metabolism systems. It is characterized by profound fatigue along with a range of other symptoms including pain, cognitive impairment, autonomic dysfunction, and sleep disturbances.. Symptoms are typically worsened by often minor physical or mental exertion referred to as post-exertional malaise (PEM)
Despite the high demand for curative options, there is currently no regulatory approved therapeutic option for ME/CFS.
Hyperbaric Oxygen Therapy (HBOT) involves breathing 100% oxygen in a pressurized chamber, typically at 1.5 to 2.5 times normal atmospheric pressure. These conditions permit a significant increment of the oxygen supply to blood and to tissues even without the contribution from hemoglobin. This may aid in conditions where improving oxygen delivery can support recovery.
It is hypothesised that, through its effect, HBOT may elicits a cascade of cellular responses that collectively may address many pathophysiological aspects of ME/CFS.
Previous Research Investigation HBOT
Previous research regarding ME/CFS and HBOT has had limitations and produced mixed results. Following the COVID-19 pandemic however, several studies, including one randomized controlled trial (RCT) and case series, investigated the potential effects of HBOT in post-COVID syndrome, which is known to have overlapping pathophysiology with ME/CFS.
Overall, the findings consistently showed improvements in quality of life, fatigue, cognitive function, neuropsychiatric symptoms, and cardiopulmonary function. Improvements have also been associated with structural changes in the brain with lasting effects up to one year and possibly longer if monitoring was to be continued.
Given the overlapping pathophysiology between Long-Covid and ME/CFS researchers recently aimed to explore the effectiveness of HBOT as a treatment for ME/CFS. Additionally structural and functional changes in the brain were also assessed using MRI technology. The overall goal being to clarify the role of HBOT in post-COVID ME/CFS and develop more evidence based treatments.
Noteworthy Mechanisms for HBOT
HBOT may stabilize hypoxia-inducible factor (HIF)-1α and thereby lead to an upregulation of enzymes for anaerobic glycolysis to sustain adenosine triphosphate (ATP) production when oxygen is low, while tempering oxidative stress over time.
Simultaneously, HIF-1α can drive the expression of growth factors like vascular endothelial growth factor (VEGF), leading to angiogenesis and improving oxygen delivery.
HBOT may modulate the immune system by reducing excessive inflammatory cytokines and promoting anti-inflammatory profiles.
What Did The Researchers Do?
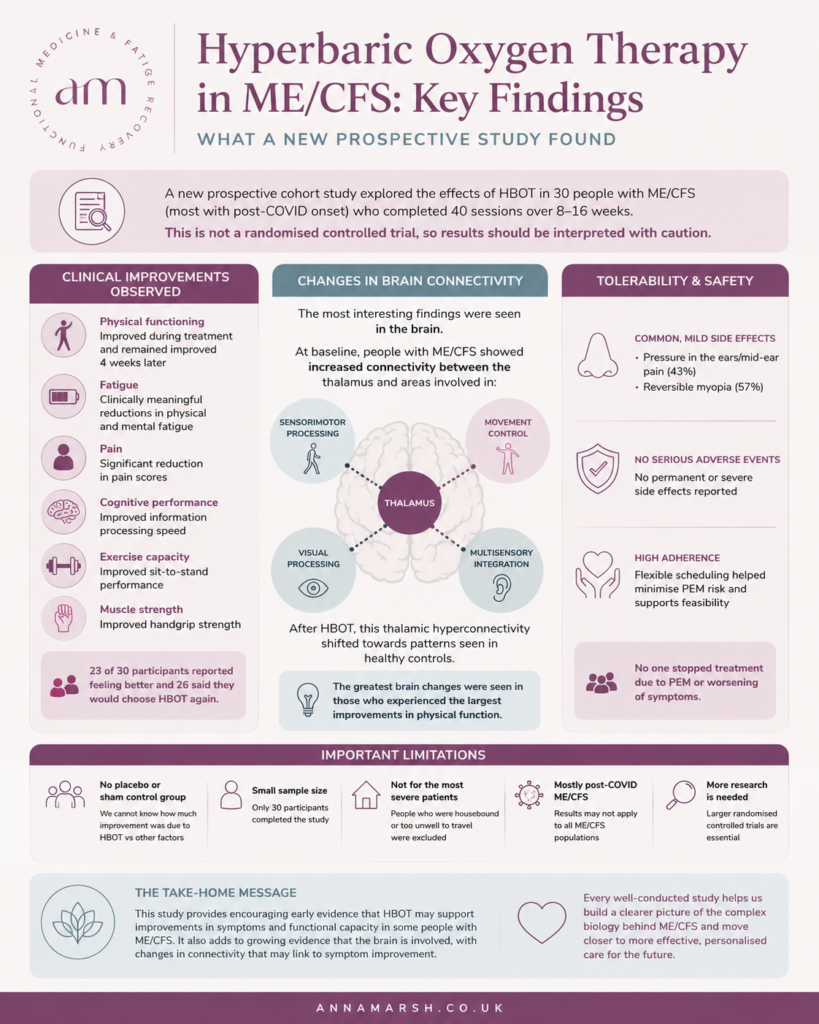
The study design was a prospective cohort study which means the study followed a specific group of people, in this case 30 patients diagnosed with ME/CFS, over a period of time. The patients had 40 HBOT sessions across 8-16 weeks and there was a follow up visit 4 weeks after the 40 sessions were completed.
The study was limited to patients who could leave their homes. In other words those who were too ill to leave their home to receive treatment were excluded and therefore we cannot draw conclusions based on this sub-set of individuals.
Participants received up to 5 sessions per week across 8-16 weeks. The protocol involved breathing 100% oxygen via a mask at 2 ATA (atmospheres absolute) for 90 minutes, with a 5 minute air break every 20 minutes.
In 27 of the 30 patients SARS-CoV-2 Infection was identified as the main trigger. The remaining 3 had a viral trigger. All individuals were classified as moderate to severe in their degree of disability. Thirteen also experienced POTS and 8 had a pre-existing autoimmune condition.
Because of the risk of PEM and worsening of symptoms due to travel to and from treatment and the need to sit upright for 90 minutes to participate in the study, the study implemented a flexible protocol where sessions could be taken across an 8-16 week period. This resulted in a high adherence rate and no early termination due to PEM.
What Did They Measure?
Questionnaires were done before treatment commenced, 4 weeks into treatment, on the final day of treatment and 4 weeks following treatment.
- A 36 item short form survey (SF-36) was used to assess health related quality of life.
- Fatigue was evaluated using the Chalder Fatigue Scale (CFQ).
- Handgrip strength and orthostatic dysfunction were also assessed.
MRI
Patients also participated in a baseline MRI session 4 weeks prior to HBOT therapy and a follow up session within 4 weeks of concluding treatment. For the MRI portion of the study, a health control group underwent a single scan for comparison purposes.
Response To HBOT Treatment
Of 37 patients initially enrolled in the study, 1 was unable to complete due to upper respiratory tract infections and 6 discontinued due to pressure-related pain in the sinuses and ears or a feeling of tightness and anxiety.
It took on average 13 weeks for the patients to complete all the sessions. Breaks were required between sessions to prevent symptom exacerbation.
23 of the 30 patients reported subjective improvement and 26 would receive HBOT treatment again in the future.
Some side effects were reported such as:
- Feeling of pressure in the ear or mid-ear pain (43%)
- Reversible myopia (57%)
- No permanent or severe side effects were reported
- None discontinued treatment due to PEM or worsening symptoms
The greatest improvement in their quality of life assessment was observed on the last day. Four weeks after treatment, there was still a significant improvement from baseline.
The improvements reflected improved physical functioning including a significant reduction in pain and both physical and mental fatigue,
Functional Tests also showed improvements in:
- Exercise capacity
- Cognitive performance and information processing speed
- Handgrip strength
- Orthostatic Tolerance Test (1 minute sit to stand)
Brain Imaging
MRI findings showed thalamic hyperconnectivity at baseline which shifted more towards the pattern observed in health controls following the HBOT sessions. Baseline increased connectivity, which may reflect impaired filtering, heightened sensory gain, or compensatory over-engagement of thalamocortical circuits. These are brain regions which have previously been implicated in fatigue, sensory overload and motor slowing in ME/CFS.
There was some suggestion that clinical improvement in physical functioning may be associated with changes in thalamic regulation.
HBOT and ME/CFS Study Conclusions
This observational study suggests that HBOT may improve physical functioning, reduce pain and fatigue severity, and enhance exercise capacity, muscle strength, and information processing speed in a subset of ME/CFS patients.
Due to the flexible protocol and high adherence rate and the fact that the majority of participants said that they would use HBOT again the researchers deemed HBOT a feasible and acceptable treatment for ME/CFS.
The primary outcome of the study was the improvement in the SF-36, including reduction in fatigue and pain. Self reported physical functioning improved during treatment and at the 4 week follow up with 37% of participants experiencing improvements which were deemed “clinically meaningful”.
The study mentioned that improvements in SF-36 must be interpreted cautiously as previous studies have suggested that changes can reflect natural fluctuations and not necessarily important clinical improvements.
However, there were also non-self reported outcomes from the study which were meaningful; handgrip testing and sit to stand orthostatic intolerance testing showed significant improvement from pre- and post-HBOT.
The study concluded by saying that they observed therapeutic effects on several core symptoms of ME/CFS and that consistent improvements across multiple symptom domains, together with high adherence to the demanding treatment protocol and favorable tolerability, further support the feasibility and clinical relevance of HBOT in this patient population.
Study Limitations
The findings of this study were encouraging. However, all research has limitations and it is important to note the following.
The study utilised a small sample size and, being a prospective cohort study, there were no controls – apart from the control group used for the brain imaging.
Severely affected housebound patients were excluded from the trial. Additionally all participants had a viral trigger (i.e. COVID or otherwise). Therefore we cannot conclude safety and efficacy in more severely impacted sub-groups or sub-groups with a different clinical picture.
Ongoing questions remain regarding optimal number of sessions and frequency of HBOT sessions and the durability of reported effects However, a second cohort is currently underway to answer some of these questions including a shortened 20 session protocol which also includes additional markers including perfusion analysis, inflammatory markers, and endothelial function tests.
Anna’s Hot take
Personally I found the outcomes of this study encouraging. It is always great to see more research that supports the ME/CFS community. My concerns in clinical practice for recommending HBOT is always clinical tolerance. The first concern is often not: Will this help my client. Instead: What are the risks of this making someone worse?
Although the sample size is small, for those who are able to manage the travel and tolerate the sessions, the study seems to demonstrate that this may be a fairly safe intervention.
As a precaution I would always want someone to have a general sense of stability and have mastered the foundations of Nervous System Regulation, Blood Sugar Management, Pacing, Sleep and Managing Inflammation in the body (the things we cover in the Nurturing Resilience Membership).
With these in place, there may possibly be scope for more guaranteed success with HBOT.
What now?
If you’re navigating ME/CFS or Long Covid and looking for a science-based, whole-person approach to recovery, you may find support inside my Nurturing Resilience Membership, where we explore many of these foundational strategies in greater depth and discuss emerging research as it develops.